



Episode Terakhir The One and Only 100 Persen Haru
retroconference.org – Episode Terakhir The One and Only 100 Persen Haru. Drama Korea The One and Only menutup kisahnya dengan…

Berita Terupdate Seputar Dunia Film
retroconference.org – Episode Terakhir The One and Only 100 Persen Haru. Drama Korea The One and Only menutup kisahnya dengan…
retroconference.org – Tema Goblin Jahat di Evil Goblins xBomb Versi 2026 Terbaru. Evil Goblins xBomb versi 2026 hadir dengan nuansa…
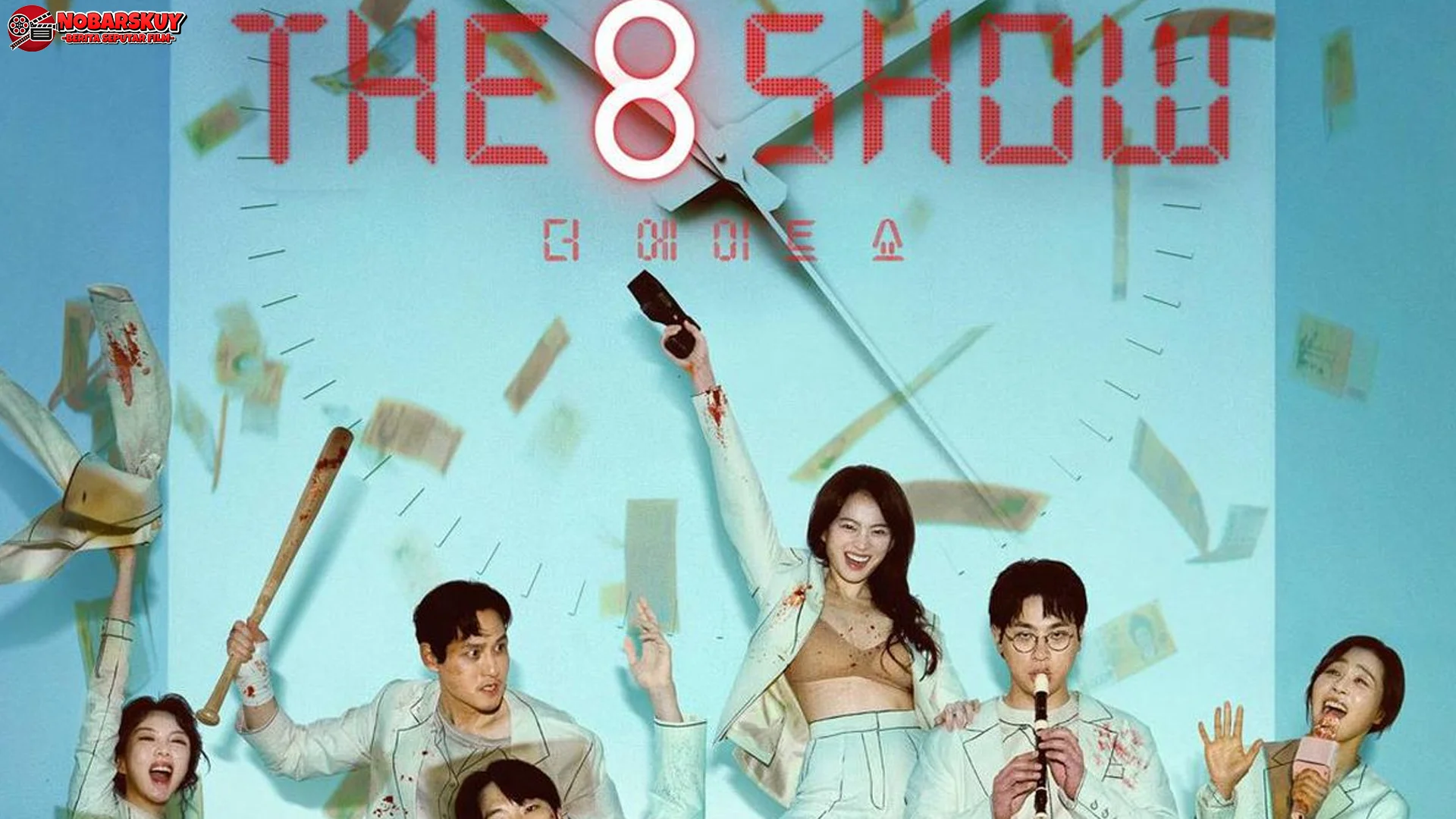
retroconference.org – Alur The 8 Show Semakin Gila di Setiap Episode Baru. Dunia drama Korea selalu menghadirkan konsep cerita yang…
retroconference.org – Shamrock Quest Sihir Dalam 5 Cara Buka Clover Langka. Shamrock Quest membawa suasana yang langsung terasa berbeda sejak…
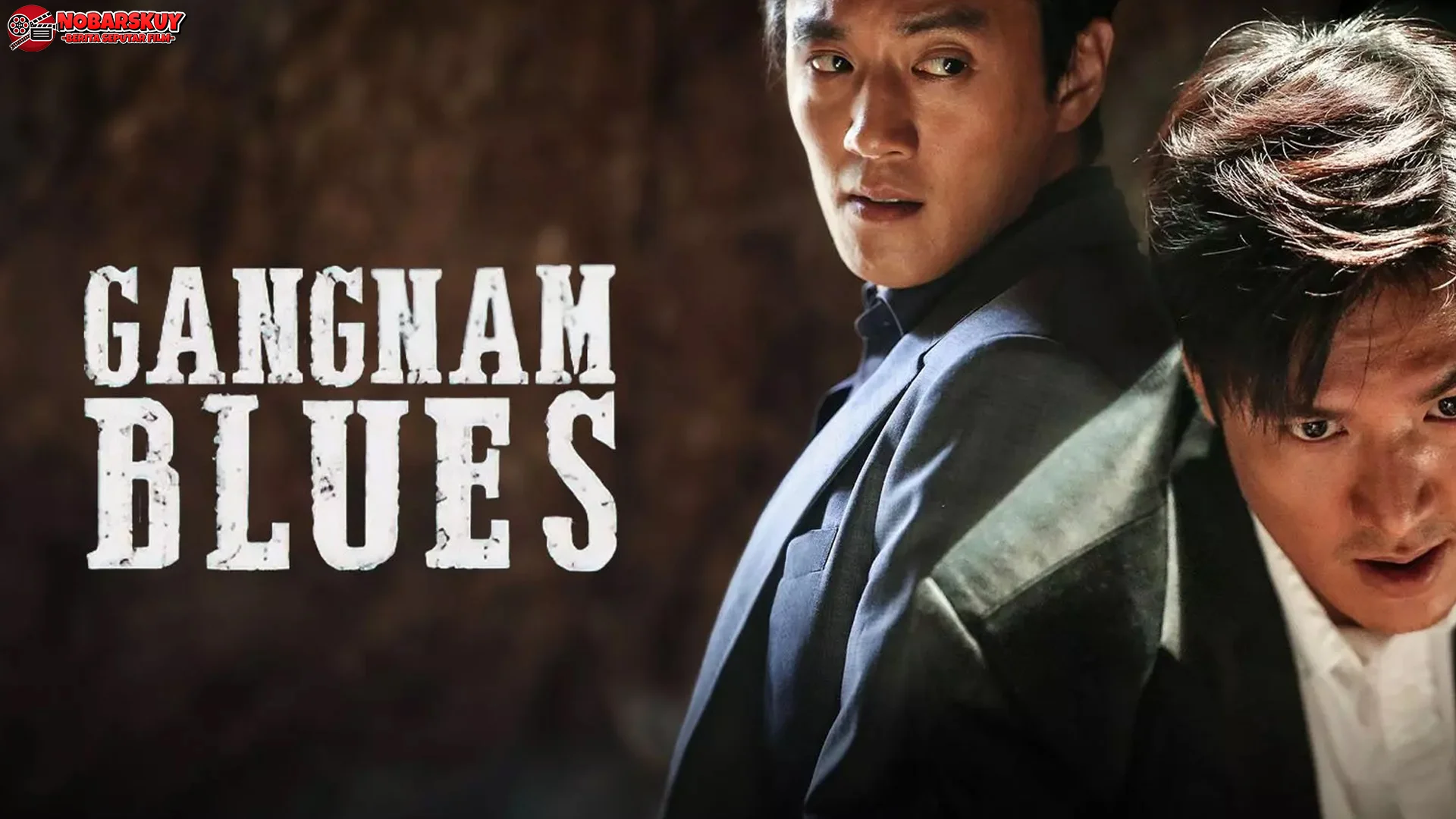
retroconference.org – Gangnam Blues Dan 4 Adegan Action Paling Brutalnya. Film Gangnam Blues membawa penonton ke dunia keras yang dipenuhi…
retroconference.org – 5 Slay Rio Fantasia Dalam Penampilannya Beneran Slay Abis. Rio Fantasia muncul sebagai game yang langsung punya karakter…
retroconference.org – Review Something in the Rain 4 Kisah Cinta Beda Usia. Drama Korea selalu punya cara sendiri untuk bikin…
retroconference.org – Dibalik Popularitas Slayers Inc Gandeng 4 yang Naik Daun Parah. Slayers Inc Gandeng 4 lagi ramai dibicarakan karena…
retroconference.org – 2 Ending Suspicious Partner yang Memuaskan Hati . Suspicious Partner dikenal sebagai drama yang membawa penonton masuk ke…
retroconference.org – True Grit Redemption Lewat 5 Tahap Tersulit Abadi Ini. True Slot Grit Redemption hadir dengan karakter yang keras…